

Abdominal obesity, also known as central obesity, is when excessive abdominal fat around the stomach and abdomen has built up to the extent that it is likely to have a negative impact on health. There is a strong correlation between central obesity and cardiovascular disease. Abdominal obesity is not confined only to the elderly and obese subjects. Abdominal obesity has been linked to Alzheimer's disease as well as other metabolic and vascular diseases.
Visceral and central abdominal fat and waist circumference show a strong association with type 2 diabetes.
Visceral fat, also known as organ fat or intra-abdominal fat, is located inside the peritoneal cavity, packed in between internal organs and torso, as opposed to subcutaneous fat, which is found underneath the skin, and intramuscular fat, which is found interspersed in skeletal muscle. Visceral fat is composed of several adipose depots including mesenteric, epididymal white adipose tissue (EWAT) and perirenal fat. An excess of visceral fat is known as central obesity, the "pot belly" or "beer belly" effect, in which the abdomen protrudes excessively. This body type is also known as "apple shaped", as opposed to "pear shaped", in which fat is deposited on the hips and buttocks.
Researchers first started to focus on abdominal obesity in the 1980s when they realized it had an important connection to cardiovascular disease, diabetes, and dyslipidemia. Abdominal obesity was more closely related with metabolic dysfunctions connected with cardiovascular disease than was general obesity. In the late 1980s and early 1990s insightful and powerful imaging techniques were discovered that would further help advance the understanding of the health risks associated with body fat accumulation. Techniques such as computed tomography and magnetic resonance imaging made it possible to categorize mass of adipose tissue located at the abdominal level into intra-abdominal fat and subcutaneous fat.
Video Abdominal obesity
Health risks
Central obesity is associated with a statistically higher risk of heart disease, hypertension, insulin resistance, and Diabetes Mellitus Type 2 (see below). With an increase in the waist to hip ratio and overall waist circumference the risk of death increases as well. Metabolic syndrome is associated with abdominal obesity, blood lipid disorders, inflammation, insulin resistance, full-blown diabetes, and increased risk of developing cardiovascular disease. It is now generally believed that intra-abdominal fat is the depot that conveys the biggest health risk.
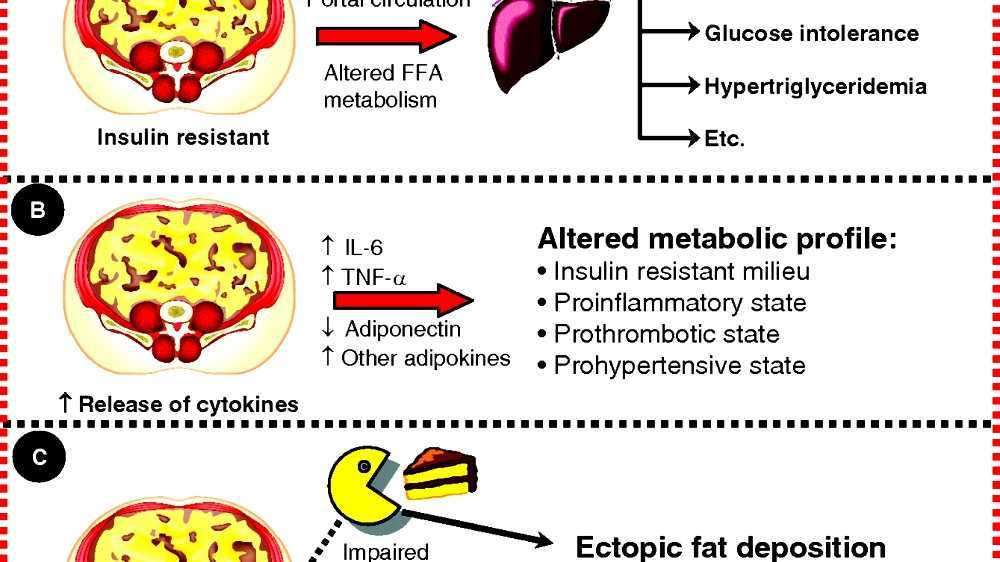
Central obesity can be a feature of lipodystrophies, a group of diseases that is either inherited, or due to secondary causes (often protease inhibitors, a group of medications against AIDS). Central obesity is a symptom of Cushing's syndrome and is also common in patients with polycystic ovary syndrome (PCOS). Central obesity is associated with glucose intolerance and dyslipidemia. Once dyslipidemia becomes a severe problem, an individual's abdominal cavity would generate elevated free fatty acid flux to the liver. The effect of abdominal adiposity occurs not just in those who are obese, but also affects people who are non-obese and it also contributes to insulin sensitivity.
Recent validation has concluded that total and regional body volume estimates correlate positively and significantly with biomarkers of cardiovascular risk and BVI calculations correlate significantly with all biomarkers of cardio-vascular risk.
Ghroubi et al. (2007) examined whether abdominal circumference is a more reliable indicator than BMI of the presence of knee osteoarthritis in obese patients. They found that it actually appears to be a factor linked with the presence of knee pain as well as osteoarthritis in obese study subjects. Ghroubi et al. (2007) concluded that a high abdominal circumference is associated with great functional repercussion.
Diabetes
There are numerous theories as to the exact cause and mechanism in Type 2 Diabetes. Central obesity is known to predispose individuals for insulin resistance. Abdominal fat is especially active hormonally, secreting a group of hormones called adipokines that may possibly impair glucose tolerance. But adiponectin which is found in lower concentration in obese and diabetic individuals has shown to be beneficial and protective in Type 2 diabetes mellitus.
Insulin resistance is a major feature of Diabetes Mellitus Type 2 (T2DM), and central obesity is correlated with both insulin resistance and T2DM itself. Increased adiposity (obesity) raises serum resistin levels, which in turn directly correlate to insulin resistance. Studies have also confirmed a direct correlation between resistin levels and T2DM. And it is waistline adipose tissue (central obesity) which seems to be the foremost type of fat deposits contributing to rising levels of serum resistin. Conversely, serum resistin levels have been found to decline with decreased adiposity following medical treatment.
Asthma
Developing asthma due to abdominal obesity is also a main concern. As a result of breathing at low lung volume, the muscles are tighter and the airway is narrower. It is commonly seen that people who are obese breathe quickly and often, while inhaling small volumes of air. People with obesity are also more likely to be hospitalized for asthma. A study has stated that 75% of patients treated for asthma in the emergency room were either overweight or obese.
Alzheimer's disease
Based on studies, it is evident that obesity has a strong association with vascular and metabolic disease which could potentially be linked to Alzheimer's disease. Recent studies have also shown an association between mid-life obesity and dementia, but the relationship between later life obesity and dementia is less clear. A study by Debette et al. (2010) examining over 700 adults found evidence to suggest higher volumes of visceral fat, regardless of overall weight, were associated with smaller brain volumes and increased risk of dementia. Alzheimer's disease and abdominal obesity has a strong correlation and with metabolic factors added in, the risk of developing Alzheimer's disease was even higher. Based on logistic regression analyses, it was found that obesity was associated with an almost 10-fold increase risk of Alzheimer's disease.
Maps Abdominal obesity
Causes
The currently prevalent belief is that the immediate cause of obesity is net energy imbalance--the organism consumes more usable calories than it expends, wastes, or discards through elimination. Some studies indicate that visceral adiposity, together with lipid dysregulation and decreased insulin sensitivity, is related to the excessive consumption of fructose. Greater meat consumption has also been positively associated with greater weight gain, and specifically abdominal obesity, even when accounting for calories. Other environmental factors, such as maternal smoking, estrogenic compounds in the diet, and endocrine-disrupting chemicals may be important also. Obesity plays an important role in the impairment of lipid and carbohydrate metabolism shown in high-carbohydrate diets. It has also been shown that quality protein intake during a 24-hour period and the number of times the essential amino acid threshold of approximately 10 g has been achieved is inversely related to the percentage of central abdominal fat. Quality protein uptake is defined as the ratio of essential amino acids to daily dietary protein.
Visceral fat cells will release their metabolic by-products in the portal circulation, where the blood leads straight to the liver. Thus, the excess of triglycerides and fatty acids created by the visceral fat cells will go into the liver and accumulate there. In the liver, most of it will be stored as fat. This concept is known as 'lipotoxicity'.
Hypercortisolism, such as in Cushing's syndrome, also leads to central obesity. Many prescription drugs, such as dexamethasone and other steroids, can also have side effects resulting in central obesity, especially in the presence of elevated insulin levels.
The prevalence of abdominal obesity is increasing in western populations, possibly due to a combination of low physical activity and high-calorie diets, and also in developing countries, where it is associated with the urbanization of populations.
Waist measurement is more prone to errors than measuring height and weight. It is recommended to use both standards. BMI will illustrate the best estimate of your total body fatness, while waist measurement gives an estimate of visceral fat and risk of obesity-related disease.
Alcohol consumption
A study has shown that alcohol consumption is directly associated with waist circumference and with a higher risk of abdominal obesity in men, but not in women. Excluding energy under-reporters slightly attenuated these associations. After controlling for energy under-reporting, it was observed that increasing alcohol consumption significantly increased the risk of exceeding recommended energy intakes in male participants - but not in the small number of female participants (2.13%) with elevated alcohol consumption, even after establishing a lower number of drinks per day to characterize women as consuming a high quantity of alcohol. Further study is needed to determine whether a significant relationship between alcohol consumption and abdominal obesity exists among women who consume higher amounts of alcohol.

Diagnosis
There are various ways of measuring abdominal obesity including:
- Absolute waist circumference (>102 cm (40 in) in men and >88 cm (35 in) in women)
- Waist-hip ratio (the circumference of the waist divided by that of the hips of >0.9 for men and >0.85 for women)
- Waist-to-height ratio
- Sagittal Abdominal Diameter
In those with a BMI under 35, intra-abdominal body fat is related to negative health outcomes independent of total body fat. Intra-abdominal or visceral fat has a particularly strong correlation with cardiovascular disease.
BMI and waist measurements are well recognized ways to characterize obesity. However, waist measurements are not as accurate as BMI measurements. For this reason, it is recommended to use both methods of measurements.
While central obesity can be obvious just by looking at the naked body (see the picture), the severity of central obesity is determined by taking waist and hip measurements. The absolute waist circumference 102 centimetres (40 in) in men and 88 centimetres (35 in) in women) and the waist-hip ratio (>0.9 for men and >0.85 for women) are both used as measures of central obesity. A differential diagnosis includes distinguishing central obesity from ascites and intestinal bloating. In the cohort of 15,000 people participating in the National Health and Nutrition Examination Survey (NHANES III), waist circumference explained obesity-related health risk better than the body mass index (or BMI) when metabolic syndrome was taken as an outcome measure and this difference was statistically significant. In other words, excessive waist circumference appears to be more of a risk factor for metabolic syndrome than BMI. Another measure of central obesity which has shown superiority to BMI in predicting cardiovascular disease risk is the Index of Central Obesity (waist-to-height ratio - WHtR), where a ratio of >=0.5 (i.e. a waist circumference at least half of the individual's height) is predictive of increased risk. Another diagnosis of obesity is the analysis of intra-abdominal fat having the most risk to one's personal health. The increased amount of fat in this region relates to the higher levels of plasma lipid and lipoproteins as per studies mentioned by Eric Poehlman (1998) review. An increasing acceptance of the importance of central obesity within the medical profession as an indicator of health risk has led to new developments in obesity diagnosis such as the Body Volume Index, which measures central obesity by measuring a person's body shape and their weight distribution. The effect of abdominal adiposity occurs not just in those who are obese, but also affects people who are non-obese and it also contributes to insulin sensitivity
Index of central obesity
Index of Central Obesity (ICO) is the ratio of waist circumference and height first proposed by a Parikh et al. in 2007 as a better substitute to the widely used waist circumference in defining metabolic syndrome. The National Cholesterol Education Program Adult Treatment Panel III suggested cut off of 102 cm (40 in) and 88 cm (35 in) for males and females as a marker of central obesity. The same was used in defining metabolic syndrome. Misra et al. suggested that these cutoffs are not applicable among Indians and the cutoffs be lowered to 90 cm (35 in) and 80 cm (31 in) for males and females. Various race specific cutoffs were suggested by different groups. The International Diabetes Federation defined central obesity based on these various race and gender specific cutoffs. The other limitation of waist circumference is that it can not be applied in children.
Parikh et al. looked at the average heights of various races and suggested that by using ICO various race- and gender-specific cutoffs of waist circumference can be discarded. An ICO cutoff of 0.5 was suggested as a criterion to define central obesity. Parikh et al. further tested a modified definition of metabolic syndrome in which waist circumference was replaced with ICO in the National Health and Nutrition Examination Survey (NHANES) database and found the modified definition to be more specific and sensitive.
This parameter has been used in the study of metabolic syndrome and cardiovascular disease.
Sex differences
50% of men and 70% of women in the United States between the ages of 50 and 79 years now exceed the waist circumference threshold for central obesity.
When comparing the body fat of men and women it is seen that men have close to twice the visceral fat as that of pre-menopausal women.
Central obesity is positively associated with coronary heart disease risk in women and men. It has been hypothesized that the sex differences in fat distribution may explain the sex difference in coronary heart disease risk.
There are sex-dependent differences in regional fat distribution. In women, estrogen is believed to cause fat to be stored in the buttocks, thighs, and hips. When women reach menopause and the estrogen produced by ovaries declines, fat migrates from their buttocks, hips, and thighs to their belly.
Males are more susceptible to upper-body fat accumulation, most likely in the belly, due to sex hormone differences. Abdominal obesity in males is correlated with comparatively low testosterone levels. Testosterone administration significantly increased thigh muscle area, reduced subcutaneous fat deposition at all levels measured, but slightly increased the visceral fat area.
Even with the differences, at any given level of central obesity measured as waist circumference or waist to hip ratio, coronary artery disease rates are identical in men and women.

Prevention and treatments
A permanent routine of exercise, eating healthily, and, during periods of being overweight, consuming the same number or fewer calories than used will prevent and help fight obesity. A single pound of fat yields approximately 3500 calories of energy (32 000 kJ energy per kilogram of fat), and weight loss is achieved by reducing energy intake, or increasing energy expenditure, thus achieving a negative balance. Adjunctive therapies which may be prescribed by a physician are orlistat or sibutramine, although the latter has been associated with increased cardiovascular events and strokes and has been withdrawn from the market in the United States, the UK, the EU, Australia, Canada, Hong Kong, Thailand, Egypt and Mexico.
A 2006 study published in the International Journal of Sport Nutrition and Exercise Metabolism, suggests that combining cardiovascular (aerobic) exercise with resistance training is more effective than cardiovascular training alone in getting rid of abdominal fat. An additional benefit to exercising is that it reduces stress and insulin levels, which reduce the presence of cortisol, a hormone that leads to more belly fat deposits.
Self-motivation by understanding the risks associated with abdominal obesity is widely regarded as being far more important than worries about cosmetics. In addition, understanding the health issues linked with abdominal obesity can help in the self-motivation process of losing the abdominal fat. As mentioned above, abdominal fat is linked with cardiovascular disease, diabetes, and cancer. Specifically it's the deepest layer of belly fat (the fat you cannot see or grab) that poses health risks, as these "visceral" fat cells produce hormones that can affect health (e.g. increased insulin resistance and/or breast cancer risk). The risk increases considering the fact that they are located in the proximity or in between organs in the abdominal cavity. For example, fat next to the liver drains into it, causing a fatty liver, which is a risk factor for insulin resistance, setting the stage for Type 2 diabetes.
In the presence of diabetes mellitus type 2, the physician might instead prescribe metformin and thiazolidinediones (rosiglitazone or pioglitazone) as antidiabetic drugs rather than sulfonylurea derivatives. Thiazolidinediones may cause slight weight gain but decrease "pathologic" abdominal fat (visceral fat), and therefore may be prescribed for diabetics with central obesity. Thiazolidinedione has been associated with heart failure and increased cardiovascular risk; so it has been withdrawn from the market in Europe by EMA in 2010.
Low-fat diets may not be an effective long-term intervention for obesity: as Bacon and Aphramor wrote, "The majority of individuals regain virtually all of the weight that was lost during treatment." The Women's Health Initiative ("the largest and longest randomized, controlled dietary intervention clinical trial") found that long-term dietary intervention increased the waist circumference of both the intervention group and the control group, though the increase was smaller for the intervention group. The conclusion was that mean weight decreased significantly in the intervention group from baseline to year 1 by 2.2 kg (P<.001) and was 2.2 kg less than the control group change from baseline at year 1. This difference from baseline between control and intervention groups diminished over time, but a significant difference in weight was maintained through year 9, the end of the study.

Society and culture
Myths
There is a common misconception that spot exercise (that is, exercising a specific muscle or location of the body) most effectively burns fat at the desired location, but this is not the case. Spot exercise is beneficial for building specific muscles, but it has little effect, if any, on fat in that area of the body, or on the body's distribution of body fat. The same logic applies to sit-ups and belly fat. Sit-ups, crunches and other abdominal exercises are useful in building the abdominal muscles, but they have little effect, if any, on the adipose tissue located there.
Colloquialisms
Several colloquial terms used to refer to central obesity, and to people who have it, refer to beer drinking. However, there is little scientific evidence that beer drinkers are more prone to central obesity, despite its being known colloquially as "beer belly", "beer gut", or "beer pot". One of the few studies conducted on the subject did not find that beer drinkers are more prone to central obesity than nondrinkers or drinkers of wine or spirits. Chronic alcoholism can lead to cirrhosis, symptoms of which include gynecomastia (enlarged breasts) and ascites (abdominal fluid). These symptoms can suggest the appearance of central obesity.
Deposits of excess fat at the sides of one's waistline are commonly referred to as "love handles".
Economics
Researchers in Copenhagen examined the relationship between waist circumferences and costs among 31,840 subjects aged 50-64 years of age with different waist circumferences. Their study showed that an increase in just an additional centimetre above normal waistline caused a 1.25% and 2.08% rise in health care costs in women and men respectively. To put this in perspective, a woman with a waistline of 95 cm. and without underlying health problems or co-morbidities can incur economic costs that are 22%, or 397 USD, higher per year than a woman with a normal waist circumference.

See also
- Bariatrics, the branch of medicine that deals with the causes, prevention, and treatment of obesity
- Lipoatrophy, the term describing the localized loss of fat tissue
- Lipodystrophy, a medical condition characterized by abnormal or degenerative conditions of the body's adipose tissue.
- Panniculus, hanging belly fat
- Sagittal Abdominal Diameter (SAD), a measure of visceral obesity
- Steatosis, also called fatty change, fatty degeneration or adipose degeneration

References
Further reading
- Griesemer, Rebecca Lynn (July 25, 2008). Index of Central Obesity as a Parameter to Evaluate Metabolic Syndrome for White, Black, and Hispanic Adults in the United States (Master's thesis). Georgia State University.
- Lee, Kayoung; Song, Yun-Mi; Sung, Joohon (2008). "Which Obesity Indicators Are Better Predictors of Metabolic Risk?: Healthy Twin Study". Obesity. 16 (4): 834-40. doi:10.1038/oby.2007.109. PMID 18239595.
- Shao, J.; Yu, L.; Shen, X.; Li, D.; Wang, K. (2010). "Waist-to-height ratio, an optimal predictor for obesity and metabolic syndrome in Chinese adults". The Journal of Nutrition, Health & Aging. 14 (9): 782-5. doi:10.1007/s12603-010-0106-x. PMID 21085910.
Source of the article : Wikipedia
